December 30, 2022
Open Letter to Dartmouth College’s President Hanlon, Members of the Board of Trustees, and the Dartmouth Community1,
One death from a vaccine used to be too many. Today, there are over 33,000 reported deaths from the COVID-19 vaccines in the U.S. vaccine injury reporting system (VAERS), multiples larger than all the previously reported vaccine deaths since 1990 (Figure 1)2. Previous (pre- COVID) analysis suggest the VAERS under-reporting is 10x-40x+. The close proximity of reported deaths to the timing of the injections, most happening within just a few of days, is quite evident (Figure 2). This is only a fraction of the global total, as populations all over the world are experiencing significantly higher excess mortality following the introduction of certain of the COVID-19 vaccines in early 2021.
Figure 1: All Deaths Reported to VAERS by Year
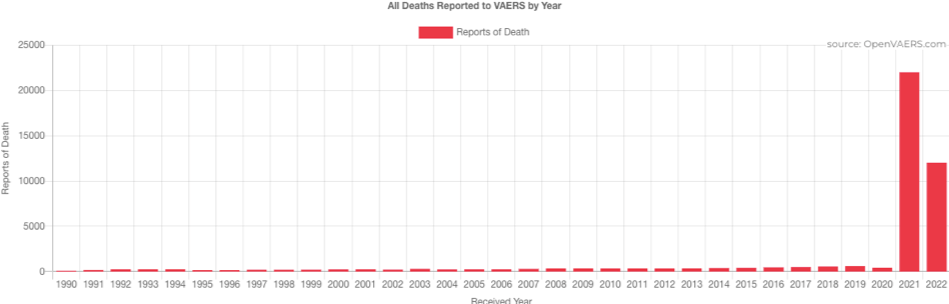
Figure 2: VAERS COVID Vaccine Reports of Death by Days to Onset (All Ages)

Our intent in writing this open letter is to raise awareness of the potential harms of the COVID-19 vaccines to help ensure that children and adults do not continue to be coerced into potentially harmful and deadly injections to gain an education or earn a living, and that those promoting such injections recognize the potential harm and cease such endorsements. We wish to see those who have been injured or have loved ones who passed gain legal accountability and restitution. We hope to ensure that the events of the last few years are not repeated.
We are calling on Dartmouth policymakers (and others this letter may reach) to recognize that promoting vaccines as a school or employment requirement, even with the ability to apply for religious or medical exemption, fails to recognize that the “cure” may be worse than the virus itself for most people, and any previously stated or perceived benefit that they would halt transmission has been proven false.
One vaccine death used to be too many. This is not a political issue, it is a human issue. We must acknowledge that these experimental “vaccines,” or more properly called gene therapy injections, are very different than previous vaccines. They should have been tested, scrutinized, marketed, and monitored as such. They were not. Now they may be one of the leading cause of non-COVID excess mortality in many of the most heavily vaccinated countries. Turning a blind eye, perhaps previously inadvertent, from now on willful, is immoral and unacceptable. The College’s COVID-19 vaccination policy should be rescinded in its entirety immediately pending further investigation.
“Suspend the mRNA jabs now. Right now they are all risk with close to zero benefit,” tweeted Dr. Aseem Malhotra3 on December 23, 2022.
Most in the medical community, like Dr. Malhotra, a prominent UK cardiologist who in October 2022 addressed the UK Parliament4 with his urgent concerns regarding COVID-19 vaccine safety, could not have imagined that a vaccine could do this type of harm. In fact, he (and many others) went on television to recommend the vaccine in his attempt to combat vaccine hesitancy in the early months after its January 2021 release, after already taking the experimental mRNA shots himself. After his father, also a physician, COVID-19 vaccine supporter and recipient, died of a sudden heart attack, it led Dr. Malhotra to carefully review his father’s case. The case puzzled Dr. Malhotra given his professional and personal understanding of his father’s recent health history, which did not suggest significant near-term potential for a heart-related event.
After spending months reviewing the original clinical trial and latest data, conducting his own research and detailing it in a peer-reviewed paper5, Dr. Malhotra has been very publicly and emphatically calling for the immediate halt of the COVID-19 injections after re-appearing onto the public scene in a tweet and 30-second video dated October 19, 2022, “It’s my duty as a cardiologist to urgently inform every Dr., patient & member of the public that the mRNA product is a likely contributory factor in all unexpected cardiac arrests, heart attacks, strokes, cardiac arrhythmia & heart failure since 2021 until proven otherwise6.”
“There is almost close to zero benefit now from the COVID vaccine at preventing COVID death and I’ll break that down in a second”, Dr. Malhotra said in a recent interview7. “But the serious adverse event rates, based upon the highest level quality of data, Pfizer’s and Moderna’s own randomized control trials, are unprecedented. And there are at least 1 in 800, life changing, disability, etc. And they are constant. But the benefits are almost negligible. You have to vaccinate, for example, 7,300 people over the age of 80 to prevent one COVID death.
And, when you look at other vaccines that have been pulled for harms, they are much less.
Swine flu vaccine, 1976, was suspended because it was found to cause Guillain–Barré syndrome in 1 in 100,000 people.
Rotavirus vaccine pulled in 1999 for causing a form of bowel obstruction 1 in 10,000.
We are talking from double-blinded randomized placebo control trial, at least 1 in 800 serious adverse events, and the most common of those, Drew, are clotting abnormalities. So heart attacks, strokes, clots of the lung, pulmonary embulai. So these are really serious issues.”
In reaction to Dr. Malhotra’s paper, Jay Bhattacharya, Professor of Medicine and Epidemiology at the University of Stanford, co-author of The Great Barrington Declaration stated, “Dr. Aseem Malhotra has written a detailed narrative review of the literature on the uses and abuses of the mRNA covid vaccines. Dr. Malhotra makes a good case that there is considerable heterogeneity across age groups and other comorbid conditions in the expected benefits and expected side effect profiles of the vaccine. He finds that, while there may be a case for older people to take the vaccine because the benefits may outweigh expected harm, that may not be the case for younger people. Dr. Malhotra’s paper calls for a pause in the use of the vaccine in younger people, such as the one recently adopted by Danish public health authorities and the Florida department of public health in the United States. He calls for investigation of side effect profiles of mRNA vaccines and for a halt to any vaccine mandate programs involving COVID vaccines. These papers should be considered carefully by all public health authorities who seek to adopt principles of evidence-based medicine in their recommendations to the public regarding the COVID mRNA vaccines.”9
If you have yet to hear of The Great Barrington Declaration, Dr. Bhattacharya, or Dr. Malhotra, look no further than Dr. Bhattacharya’s and his co-plaintiffs’ First Amendment lawsuit which provides a lens into the pervasive censorship of these last few years. The plaintiffs allege U.S. Government officials were colluding with big tech (e.g. Twitter, Google’s YouTube, and Facebook to censor material information that directly contradicted the false narrative “safe and effective”. Tweets, accounts, videos, etc. were removed under the guise of “misinformation”. Following discovery in journalist Alex Berenson’s lawsuit with Twitter, and more recently following Elon Musk’s purchase of Twitter and release of “Twitter Files”, more of the details are beginning to emerge about such active censorship10.
An example of censorship that should cause every American to stop and consider the implications was of just one video clip from a December 2020 Senate hearing removed from YouTube after going viral with about eight million views11. In this instance, the hearing included medical experts like Dr. Pierre Kory, who were testifying to successfully treating patients at various stages of the COVID-19 disease, and about promising cheap off-patent drugs being utilized as early treatment for COVID-1912.
In Dr. Kory’s written testimony provided in the Senate13, he said, “and so, it is with great pride as well as significant optimism, that I am here to report that our group, led by Professor Paul E. Marik, has developed a highly effective protocol for preventing and early treatment of COVID-19. In the last 3-4 months, emerging publications provide conclusive data on the profound efficacy of the anti-parasite, anti-viral drug, anti- inflammatory agent called ivermectin in all stages of the disease. Our protocol was created only recently, after we identified these data.
To later make matters worse, as the general population was increasingly seeking viable alternative treatments, the FDA clamped down on use of this “wonder drug”14 in its infamous tweet on August 21, 2021, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” directed against people taking Ivermectin, one of WHO’s Most Essential Drugs and available in human pill form, not to mention over 20 studies showing strong efficacy against COVID-19 viruses and a billion doses administered safely historically as an anti-viral.
This alone should place enough doubt in a policymaker’s mind that perhaps something is not right. How could it be that something this potentially important to the global populace, in the heat of a failed pandemic response, where people suffering from the effects of a novel virus were told to stay at home and do nothing until having trouble breathing, at which point come to the hospital to be placed on a ventilator with a low probability of survival, and prior to the rollout of the unproven experimental gene therapies, could be purposely withheld from the public, its intended recipient?
The questions must be asked, how many deaths could have been prevented if Dr. Kory and his colleagues’ messages had not been censored? Who is responsible for these decisions? Why was Uttar Pradesh, India (population of about 240 million), one of the only regions in the world to take a different non-vaccine path using alternatives including Ivermectin, so successful in managing to eradicate COVID deaths, that almost nobody has even heard this in the U.S.? It’s a province almost the size of the entire 330 million U.S. population.
Senator Ron Johnson from Wisconsin is certainly doing his best to encourage discussion and investigate the situation, hosting his second Senate roundtable on December 7, 2022 to help provide the most up-to-date facts and information on COVID-19 and the adverse effects of the vaccines from notoriously censored medical and other experts.15 It was the second Senate roundtable the Senator has hosted (first in January 202216) and the second time invitations for Dr. Fauci, Dr. Walensky and others from their organizations to attend were turned down. Not a single person showed up to combat all the “mis-information”.
If the people making these decisions say they are based on “the science,” but are not willing to face the scrutiny of other scientists, then perhaps we should spend more time listening to what those other not so “fringe” scientists are saying. To our knowledge, there has never been an open (or even closed-door session) between the leading scientists from the NIH/CDC/FDA and those attending Senator Ron Johnson’s roundtable. We would encourage the College to sponsor such scientific debate so we may all get to the bottom of what the data truly show and what it implies for the health of the Community the College so valiantly wishes to support through its misguided vaccination policy.
Where there’s smoke, there’s fire. Investigations are in process, some for quite some time17, and many more facts will start to come to light. What did you know, when did you know it, and what did you do about it? These are questions that will need to be answered by policymakers in the weeks and months ahead.
The State of Florida has initiated its own investigation. On October 7th, the State of Florida’s Surgeon General Ladopo came out publicly recommending against males aged 18 to 39 from receiving mRNA COVID-19 vaccines after conducting its own study into the potential adverse events. “Those with preexisting cardiac conditions, such as myocarditis and pericarditis, should take particular caution, Ladopo advised.”18
On December 13th, Governor Ron DeSantis announced the request to the Florida Supreme Court to impanel a grand jury to investigate COVID-19 vaccine manufacturers for misrepresenting and misleading19, which on December 22nd was granted20. Florida plans to hold the medical establishment accountable by creating a grand jury to investigate mRNA shots and and their manufacturers, investigating cardiac-related deaths tied to the mRNA vaccine, and forming a Public Health Integrity Committee to oversea the medical establishment.
Following the announcement to investigate the manufacturers in Florida, Oregon State Senator Dennis Linthicum offered to share evidence from its own grand jury team’s investigation with Governor Ron DeSantis’s team.
In the letter from State Senator Linthicum he noted, “that they formed a grand jury team comprised of the Senator, Senator Kim Thatcher (R-OR), attorney Steve Joncus, retired judge and grand jury expert Paul Nally, author and grand jury expert Kelly Mordecai, death certificate data analyst John Beaudoin, RICO investigator Keith Wilkins, and Dr. Henry Ealy, lead author of two peer-reviewed papers detailing the extensive criminal fraud and someone who has been successfully treating people injured by the experimental COVID biologics for more than a year.
Since 2020, our grand jury team has been in relentless pursuit of obtaining a grand jury investigation into the rampant criminal fraud and willful misconduct by key members of federal agencies. To our knowledge, we are the first team in the county to have filed a grand jury petition on behalf of the American people complete with over 1,000 pages of substantive evidence alleging that persons within the CDC, HHS, and NVSS routinely violated multiple federal laws throughout this COVID crisis.
We are confident in the evidence we have amassed being able to prove each of our allegations and would like to do all we can to support Governor DeSantis’s efforts in petitioning a state-wide grand jury or special grand jury in Florida.
In total, our research estimates the misappropriation of US Taxpayer funds to be more than $3.5 trillion.”
Other investigations include those in the European Union, which appeared to have received a larger boost when on October 10th, a Pfizer executive admitted in EU Parliament testimony that its mRNA drug had not undergone testing for transmission, stating “we had to really move at the speed of science.”21
Shortly after this public admission, on October 14th, the European Public Prosecutor’s Office confirms “that it has an ongoing investigation into the acquisition of COVID-19 vaccines in the European Union. This exceptional confirmation comes after the extremely high public interest. No further details will be made public at this stage.”22
That same day, Cristian Terhes, Member of the European Parliament from Romania, called on EU President Ursula von der Leven to “resign her job since the EU Commission is under investigation by the EU Prosecutor. She cannot lecture states on the rule of law while she destroyed docs and text messages between herself and the Pfizer CEO over multi €billion vaccine procurement contracts.”
At this time, there remain no long-term studies23 regarding the effects of these experimental drugs and the short-term data (including medical physician and medical examiner/autopsy accounts) since their implementation beginning in early 2021 point to it being the cause of death in many of our friends and family members who recently passed, including other negative outcomes like myocarditis, blood clots, strokes, sudden cancers, sudden cardiac arrest, immunity deficits, stillborns and miscarriage, among many other known “side effects”25 26. According to Dr. Peter McCullough, leading U.S. cardiologist experienced in leading large clinical trials and one of the most published cardiologists in the world, these vaccines should have been pulled in February 2021 given the safety signals and lack of sufficient data safety monitoring and reporting.
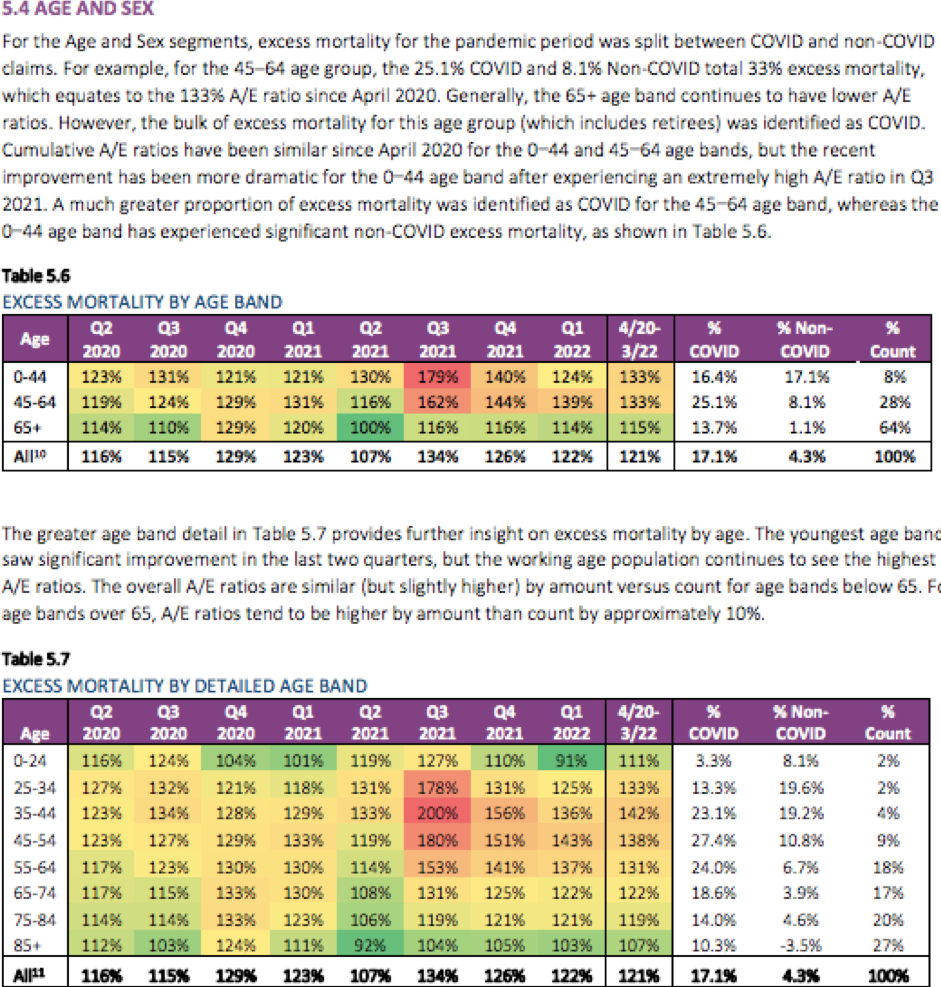
There now also appears to be sufficient data to strongly suggest a correlation between the employer (and military) vaccine mandates in Fall/Winter 2021 (Q3 2021 in Table 5.6 and 5.7 below27) and a massive spike in excess (non-COVID) mortality among the working-aged group during the time of Omicron’s less lethal wave. Ed Dowd’s, an ex-Blackrock portfolio manager, and his partner Josh Stirling’s, an ex-Sanford Bernstein #1 Institutional Investor ranked insurance analyst, review of the data points to it being particularly acute for the Group Life segment, which historically has lower mortality rates than the general population.
Today we remain in a situation where flashing red safety signals continue to be ignored and purposefully obscured. The people responsible for the public health response largely remain at the helm and maniacally focused on generating recurring revenue for manufacturers (and elected and unelected officials??) by getting the “updated” boosters, potentially lethal and injurious, into as many human arms as possible and in perpetuity (except perhaps their own).
Even now, after President Biden stated in September 2022 on 60-Minutes that the “pandemic is over”, when confronted with significant adverse data and serious concerns from established medical practitioners to the contrary, the CDC and FDA’s committee members have kept the Emergency Use Authorization (EUA) spigot flowing, just recently making the bivalent injection available for as young as 6-month olds, a drug only previously tested on 8 mice. This followed the October 20th CDC panel vote (13-0) to include the COVID-19 vaccines in the routinely recommended vaccine schedule for school-aged children30.
As we’ve seen through this pandemic, institutions all over the world have relied on the CDC’s and other public health agencies’ guidance, most without question, others as a potential immunity shield. The risk benefit ratio for children cannot possibly justify this decision31, but many states will attempt to use this recommendation to force these injections on children of parents who have already voted a resounding (but unheard) ‘NO!’ on the issue, others will automatically do so given existing statutes that reference the CDC’s “recommendations”, and many colleges and universities will point to the CDC to justify continued enforcement of their requirements.
Since the EUA approval of the shots for 6-month old through 4-years old segment in June 2022, the total uptake is an emphatically dismal 2.9% for the <2yrs and 4.7% for 2-4yrs, for those completing the primary series. Recall, the New York City Mayor and his health advisors justified keeping 100% of 2-4 year olds masked in school for months earlier this year after removing the requirements for all other age groups in large part because they did not yet have access to the vaccines.
Great societal damage and loss of life has taken place due to:
- the obstruction of true informed consent, a core medical and ethical right (see the Nuremberg Code below),
- the withholding of proper warnings, studies, and scientific discussion regarding the benefit versus risk of potential severe adverse effects of the vaccines, masking, and lockdowns,
- threats to medical practitioners’ licenses for those providing a more balanced medical opinion of the risks and benefits, which in this case contradicted the “safe and effective” narrative, created a deafening silence among physicians charged to “First, do no harm!”,
- such threats greatly hindered people’s ability to find doctors to write letters of medical exemptions, making any medical exemption much more difficult, if even possible to attain to abstain,
- attacks against simple, cost-effective alternative early prevention treatments32 that potentially invalidate EUA status, while downplaying the benefit of natural post-infection immunity,
- private and public employer and military vaccination mandates33, which helped to foster an “us against them” mentality, a form of psychological warfare, scapegoating and punishment of the “unvaccinated” non-compliant through isolation, ostracism, loss (and threat of loss) of employment, removal from duty, and loss of basic freedoms,
- improper alignment of incentives between pharmaceutical companies, their regulators, hospitals, and the media,
- select pharmacies and pharmacists willfully restricted viable off-patent, low-cost alternative drugs prescribed by physicians that could have had a significant impact on reducing negative outcomes from the COVID-19 viruses and dramatically reducing the number of severe outcomes and deaths from COVID-19,
- discussion regarding the U.S.’s history of funding gain-of-function research and the Wuhan lab-leak hypothesis were publicly and vehemently denied as to having any validity. Privately, Dr. Fauci’s and Dr. Collin’s own emails from February 2020 (only recently available in un-redacted form due to a recent FOIA request34) suggested a larger possibility that the virus (and subsequent whistleblower testimony alleges35) came from the Wuhan Institute of Virology laboratory than what the public was led to believe. This appears to imply a concerted effort to significantly downplay these questions of ‘origin’ from the public conversation very early on and throughout the pandemic.
The burden of proof is on those who continue to promote and mandate these shots. We expect this letter provides more than sufficient support to justify a halting of the College’s COVID-19 vaccination policy pending further investigation.
Urgently,
Michael (’00) and Alexis Koss
The Nuremberg Code:36
1. The voluntary consent of the human subject is absolutely essential.
This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment.
The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.
2. The experiment should be such as to yield fruitful results for the good of society, unprocurable by other methods or means of study, and not random and unnecessary in nature.
3. The experiment should be so designed and based on the results of animal experimentation and a knowledge of the natural history of the disease or other problem under study that the anticipated results will justify the performance of the experiment.
4. The experiment should be so conducted as to avoid all unnecessary physical and mental suffering and injury.
5. No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects.
6. The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.
7. Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability, or death.
8. The experiment should be conducted only by scientifically qualified persons. The highest degree of skill and care should be required through all stages of the experiment of those who conduct or engage in the experiment.
9. During the course of the experiment the human subject should be at liberty to bring the experiment to an end if he has reached the physical or mental state where continuation of the experiment seems to him to be impossible.
10. During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill and careful judgment required of him that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.
Footnotes
(1) A copy of this letter has been sent to the editor of The Dartmouth, America’s oldest college newspaper, founded 1799, in addition to other interested parties.
(3) Dr. Malhotra’s tweet dated December 23, 2022.
(4) Following such meeting, on December 13th, MP Andrew Bridgen calls for complete suspension of mRNA jab in British Parliamentary speech and references a whistleblower who stated that “a health institution is covering up clear data that the mRNA vaccines increase inflammation in the heart arteries. They are covering this up in fear of losing pharmaceutical funding. The lead of the cardiology research department has a prominent leadership role with the British Heart Association.”
(5) Has Big Pharma Hijacked Evidence Based Medicine? Cardiologist Dr. Aseem Malhotra, a fully-vaccinated UK doctor who publicly endorsed the vaccine in 2021 is now calling for a complete halt to its use following his recently published research.
Dr. Malhotra summarized his research in a recent talk that can be found here.
(6) Dr. Malhotra’s tweet dated October 19, 2022.
(7) Dr. Aseem Malhotra Promoted mRNA Vaccine, Now Warns of Heart Risks w/ Dr Kelly Victory – Ask Dr Drew
(8) On October 4, 2020, the Great Barrington Declaration was signed. “As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.” It currently has over 934,000 signatures.
(10) Dr. Fauci’s 6-hour deposition, as well as the case filings in State of Missouri ex rel. Schmitt, et al. v. Biden, et al. may be found on NCLA’s website.
(11) YouTube Cancels the U.S. Senate, by Senator Ron Johnson (February 2, 2021).
(12) See the FLCCC Alliance for its protocol for COVID-19 prevention and early outpatient protocols.
(13) Testimony of Pierre Kory, MD. Homeland Security Committee Meeting: Focus on Early Treatment of COVID-19 (December 8, 2020).
(14) Ivermectin, ‘Wonder drug’ from Japan: the human use perspective (February 10, 2011).
(15) Senate roundtable hosted by Senator Ron Johnson (December 7, 2022) COVID-19 Vaccines: What They Are, How They Work, and Possible Causes of Injuries. 10-minute summary version.
(16) COVID-19: A Second Opinion (January 24, 2022).
(17) Whistleblower Brook Jackson filed a False Claims Act Complaint on January 8, 2021 detailing her first-hand account alleging widespread Pfizer Phase 3 trial protocol and regulatory violations at the COVID-19 vaccine site where Jackson was briefly employed. The case is ongoing.
(19) Florida Gov. DeSantis requests grand jury probe of COVID-19 vaccines (December 13, 2022).
(20) Florida high court OKs grand jury probe of COVID-19 vaccines (December 22, 2022).
(21) One of the biggest selling points for getting much of the World’s population to take the experimental injections was because it would not only stop the individual from getting the infection, but also from spreading it to their loved ones, co-workers, classmates. World health and political leaders, manufacturer CEOs, mainstream media, and social media tech companies not only told the public that was the case, but used it to implement mandates and introduce COVID passports (infrastructure that remains today). Here’s the exchange between the Pfizer executive and Rob Roos, a Member of the European Parliament from the Netherlands, which Rob Roos tweeted on October 15, 2022.
(22) Politico: EU prosecutor’s office opens investigation into COVID vaccine purchases.
(23) If the drugs had been reviewed as gene therapies, they would have required more DNA-related impact studies. Clinical trials alone take six to seven years on average to complete.
(24) Increased emergency cardiovascular events among under-40 population in Israel during vaccine rollout and third COVID-19 wave (Published April 28, 2022).
(26) Pathologist Dr. Ryan Cole interviewed by Dr. Drew and Dr. Kelly Victory regarding the damage caused by mRNA vaccines, as seen under the laboratory lens (November 30, 2022).
(27) Source: Society of Actuaries.
(28) CDC Expands Updated COVID-19 Vaccines to Include Children Ages 6 Months through 5 Years.
(29) Fact check: Were new COVID-19 boosters tested in just 8 mice? Should it matter?
(30) CDC’s Advisory Committee on Immunization Practices (ACIP) recommended updates to the 2023 childhood and adult immunization schedules, which includes adding COVID-19 vaccines to the routinely recommended vaccine schedule (October 20, 2022).
(31) See recent report COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities, published December 5, 2022, which concludes booster mandates in young adults are expected to cause a net harm and University booster mandates are unethical.
(32) COVID-19 mortality risk correlates inversely with vitamin D3 status, and a mortality rate close to zero could theoretically be achieved at 50 ng/ml 25(OH)D3: Results of a systematic review and meta-analysis (Posted September 25, 2021).
(33) Supreme Court of the State of NY County of Richmond Rules NYC COVID-19 Vaccination Mandates Unconstitutional and Arbitrary and Capricious (October 24, 2022).
(34) Unredacted Emails Finally Reveal The Shocking Truth | Peak Prosperity (November 29, 2022).
(35) NY Post: Scientist with NY non-profit tied to Wuhan lab says COVID a man-made virus (December 2, 2022).
(36) Underlined sections added by authors for emphasis.
The Nuremberg Code was created in 1947 in Nuremberg, Germany, following the trial of a group of Nazi doctors accused of conducting inhumane and often deadly experiments on prisoners of concentration camps without their consent. At the conclusion of what’s also referred to as ‘The Doctors Trial’, 16 people were found guilty.
The Nuremberg Code was developed in response to the horrors of this experimentation, with the aim of protecting human subjects in medical research. The Code, and particularly its emphasis on informed consent, has had a profound impact on international human rights law and medical ethics.
The Nuremberg Code consists of 10 principles, the first of which being that the voluntary consent of the human subject is absolutely essential in any experiment on humans.
Other principles include that the experiment should be for the good of society, that all unnecessary physical and mental suffering or injury should be avoided and no experiment should be conducted if there is good reason to believe it may result in death or a disabling injury.
Disclaimer:
Any opinions expressed in this letter are those of our own and nobody else. Nothing in this letter shall be misconstrued as providing medical, legal, investment, or any other advice that may be relied upon in any way.
